Classes for the 2025 term have ended. A ritual, before each class, 4 classes per year X 12 or 13 weeks, for the last 4 years or so, has been to start with a warmup, where we chat about data in the world, or tek talk in the world, or with an information souk, mostly about things that either relate directly to the day’s topic, or the theme of the class with the odd whimsy in there for good measure. When term ends, I miss creating this weekly roundup. So Here I am, back to the space, where the early days of open data all started, on DataLibre.ca. I will endeavour to do a bit more of this to get the kinks out in terms of writing and to share, as I must say, all the things we critical data studies scholars pointed out, well, are becoming far too real, and this moment ought to be more overtly discussed, so that we do not forget as we build new data systems, and manage the old, and consider what might happen if we do not govern and protect for the wellbeing of people and sentient beings.
To start, today, I came across a knitting clock, it is not a new piece, but one, that materializes time, and there are no data without time. I was once asked if data have an essence, I still think about that question, the best I can do for now is to say that there are many components and attributes to the whole and the parts of the assemblages that constitute data. There is no doubt, however, that time is one of these components, and of course data are data when they are recorded some how, and the database need not be a computer. So I come back with serendipity and whimsy with this lovely piece by Siren Elise Wilhelmsen and her 365 KNITTING CLOCK.
"365 Knitting Clock stitches time as it passes by. It knits 24 hours a day, one year at the time, presenting the physical representation of time as a creative and tangible force. After 365 days the clock has turned the passed year into a two-meter long scarf. Now the past can be carried out into the future and the upcoming year is hiding in a new spool of thread, still unknitted."
The Civil Society Commitments we submitted and discussed, were developed in consultation with civil society disabled people’s organizations, experts and advocates with lived experience. It was the first time that such a group had been brought together to specifically discuss data about disabled people in Canada.
After the meeting, the civil society representatives met, and recommended an additional commitment and refined the 7 point Data For Results on Disability Commitment as posted below, that was presented to government. We also reached out to those who sent their regrets for their input. It was great to have these key experts, people with lived experience and disabled people civil society organizations at the table. This was no small feat given the context of the pandemic and the front line priorities these organizations and people have.
We then formally asked that these Refined Commitments be shared with government of Canada counterparts in an email. In that correspondence we offered to look at a draft, and or to discuss ideas. It is conventional to discuss draft commitments.
Unfortunately, the Government of Canada actors responsible for this commitment did not discuss their proposed commitments prior to the public consultation process, and as you can see here, the Government’s proposal does not resemble what civil society actors requested. The Government’s draft commitment does however resemble the 2021 Federal Budget announcement on disagregated data, and new additions that just came in this afternoon, are a list of work government was already doing, thus these do not consitutue new commitments. It is great that this work is beind done, but these do not address the request that was made. (see below Civil Society Commitments 1 & 2)
As per the process, we formally submitted our disapointment to the Government of Canada proposal in an email, and we did so today again, and we have submitted comments as part of the online consultation process which you can find here and I have posted images below. We hope that this part of the process works, and that our questions and comments will be responded to. You can submit comments to!
We also hope that we will be able to work together on addressing how disabled people are unseen and generally unacounted for in government statistics, government data and administrative data, let alone open data, and that when they are, they are often misclassified or overly surveyed and audited in programs and taxation as they are often identified as outliers. Also, that data will be collected about topics and issues of importance to disabled people, in the spirit of Nothing about us with out us!
We believe the Government operated with good intentions, and we hope to be able to work together to fulfill the requests from civil society and, that our commitments will become policy and that we can have meaningful dialogue to co-create open government policy as per the process.
Preamble
Data for Results:Data about People with Disabilities
MSF Civil Society actors identified a significant data deficit regarding the living conditions and well-being of people with disabilities in Canada. These historical and systemic inequities became more visible and problematic throughout COVID-19 pandemic response. Existing data are outdated, insufficient, difficult to find and do not address systemic issues.
People with disabilities are counted as part of the Employment Equity Act in terms of employment in the Federal Government, there is a new Act to ensure a barrier-free Canada, which has led to the creation of a Canadian Accessibility Standards Development Organization (CASDO), the Canadian Survey on Disability (CSD) targets people who are 15 years and over on Census day. These are to be lauded, but there remains an absence of data about the living conditions of this group of people in terms of individual residences and most especially collective dwellings which more often than not involves state support. There is also a lack of any national understanding of how this group of people in Canada are faring and when in collective dwellings, how much freedom is afforded in terms of movement. This would be the responsibility of Statistics Canada, the CASDO, and the Public Health Agency of Canada (PHAC).
Currently there is no one statistical unit responsible for the collection of data, surveys and administrative data about people with disabilities. There is no national dataset nor a typology of collective residences and collective care facilities such as group homes, home care, and respite care. There are no unique classification systems, and the General Social Survey and the Census do not survey people with disabilities where they live, missing those who live in institutions and custodial housing. We also know little of the employment, education, health, and economic status and wellbeing of this group of Canadians. This is a first step to knowing more, and to inform policies, programs and services. Internationally this group of people are underrepresented, invisible and unseen in Open Data priorities. We hope to also address this international Open Government and Open Data gap.
Multi-Stakeholder Forum Civil Society Commitment Requests on the topic of Open Data For Results – Disability:
Data for Results – Disability Civil Society Commitment 1:
• We would like the following 7 step Data For Results process on Disability commitment:
1. Disability Data Inventory – Conduct a cross government of Canada inventory to identify data, surveys, administrative data, program and service data, models, crowdsourcing data collection programs about disabled people, including their social and material lived experience. This would include methodological guides, data dictionaries, classification systems & taxonomies, standards, etc. as well as data owners, and how the data are used in decision making and reporting. 2. Analyze – Analyze the inventory and identify data gaps and issues with disability civil society actors and experts in and outside of government. This includes identifying risks related to automated decision making, validity of the data, assessment of proxies, bias and models of disability. Also, with great attention to the potential ramifications of data to the lives of disabled people i.e. disabled people are often audited more by the CRA as their lives do not follow traditional life courses. 3. Publish – The results of the inventory and later the analysis of the inventory on the Open Government Website and publish any data that can be made open in the open data portal with accompanying documentation. This can be a type of clearinghouse on disability, including laws, regulations, official reporting, etc. 4. Collect – Develop procedures to ameliorate existing datasets, and work with Civil Society actors and experts in and outside of government to produce and collect new data with responsible authorities, keeping in mind the risks discussed earlier. 5. Publish – New, current, and historical existing data on the Government of Canada Open Data portal and also, for those data that cannot be open data, these ought to be listed with details and a contacting authority. 6. Act – Data for Results is about informing public policy, programs and services to address inequities and the social and material conditions of disabled people, to assess impact and outcomes of regulation, to mitigate ableism and to improve data collection, dissemination and processes including impact and oversight, while also creating affirmative indicators related to participation in Canadian life and the workforce. Impact metrics will be required to monitor progress. 7. Report Results – Report policy, program and service improvements and outcomes.
Data for Results – Disability Civil Society Commitment 2:
Open Government Commitment by Government of Canada
Update – Wereceived notice at 14:00 YOW time, that the following was forgottent in the Government Consulation Document
Just added list of datasets!
My submitted comments about this oversight are as follows:
“The addition of 3.7 onward, just now on a Friday afternoon before an election, is great, but these do not constitute Open Government Commitments, as these are the usual business of Government, some of the surveys should not have been cancelled in the first place, and these were things Government had already committed to. We are glad that you are going to do them. Also they have just been added on the last days of the consultation. In addition, some of these surveys do not sample disabled people living in collective dwellings such as domiciliary institutions, the living arrangements for many disabled people, which means it will miss many resulting in a gross under count and under representatio, especially people with developmental disabilities and potentially the elderly with disabilities who live in elder care homes, and any other disabled people relegated to prisons because of inadequate mental institutions, and others with developmental disabilities in mental institutions because of a lack of other forms of care.
We of course, continue to hope that our group of civil society actors will be consulted and an advisory board will be constituted with the people and organizations who helped shape and endorse the civil society submitted commitments.
Part of the issues identified by civil society, are these types of data gaps in existing counting systems, including a clear lack of typologies and classification systems about foundational issues such as living arrangements and dwelling types.
Finally, as is the case with Indigenous people, there ought to be systems developed by and with disabled people as the current deficit indicators are not useful, and what of data that are meaningful to disabled people?
Again, we are most willing to work with you. And we hope that our call for an inventory, the analysis of the data from that inventory, and an advisory group can be set up in an official capacity so that we do this work together. We look forward to your thoughts on this. We have posted our observations and requests here as comments to this document and also here https://www.datalibre.ca/2021/08/13/open-data-for-results-disability/.
Also note, that the groups we worked with as part of this process, expected their contribution in terms of the development of commitments to be enough, they did not expect to have to come back to a website and also have to reiterate what they have already share with you. Thus we did!
Again, we believe the Government has good intentions, but in the absence of dialogue with us, missed what we were proposing and why. The Open Government process involves meaningful engagement, and new commitments beyond usual government business. I am sure we will be able to help you formulate a commitment that is new, and one that is meaningful to disabled people in Canada.”
Megan Linton (Sociology) the Tracing COVID-19 Data project’s critical disabilities studies expert supported by Kit Chokly (Communications) our data intersectionality expert and designer, have been leading the charge on making public the data invisility of people living in custodial institutions. The backgrounder is available here, and in essence we are trying to compile, with disability and open data advocates across the country, a foundational dataset so that these folks can be seen in policy and in action.
Megan, in addition to being an up-and-coming scholar, is also a person with the lived experience of a disabled person has been in the news talking about these invisibilities. Today she was interviewed by CBC’s Alan Neal on All in a Day
The research team is digging for information to compile into a database with the Canadian Open Data Society, GO Open Data, and Open North and several people in the disabled people’s community and volunteers at large.
We were invited today to share the work we are doing on the Tracing COVID-19 Data project to the Ottawa Local Immigration Partnership (OLIP) Health and Wellbeing Sector Table Meeting. This is an amazing group of dedicated actors from the Social Sector, the City, Health Sector, Education Sector, Police and Equity seeking groups that work toward the promotion of equality in Ottawa. One of their Theory of Change Domain Areas is Equity Data, and you can read more about OLIP’s work here.
I was just awarded a small but not insignificant award as part of the Carleton University COVID-19 Rapid Response Research Grants. Below is a description of what I will be up to, along with some great students and expert advisors. I will share everyone’s names later. Results of the work will be published here as it becomes available! Stay tuned. Also, let me know if you want to contribute in any way! Tracey dot Lauriault at Carleton dot CA
Research Summary
There is much official COVID-19 data reporting by federal, provincial, territorial and Indigenous Communities. As the pandemic evolves, and more information comes to light, there is a call to add data attributes about Indigenous, Black and Racialized groups and of the affected labour force, and to report where cases predominate. The pandemic also revealed that foundational datasets are missing, such as a national list of elder care homes, maps of local health regions and data about the digital divide. This project will embrace technological citizenship, adopt a critical data studies theoretical framework and a data humanitarian approach to rapidly assess data shortfalls, identify standards, and support the building of infrastructure. This involves training students, conducting rapid response research, developing a network of experts, learning by doing and a transdisciplinary team of peer reviewers to assess results. The knowledge will be mobilized in open access blog posts, infographics, policy briefs and scholarly publications.
Research challenge:
Official COVID-19 public heath reports by Federal, Provincial, and Territorial (F/P/T) and First Nation Communities are uneven and there are calls to improve them ( 1 CBC News, Toronto Star). Asymmetries can be attributed to dynamically evolving challenges associated with the pandemic, such as working while practicing social distancing; jurisdictional divisions of power in terms of health delivery; and responding to a humanitarian crisis, where resources are stretched and infrastructures are splintered (i.e. digital divide, nursing home conditions).
The Harvard Humanitarian Initiative (HHI) developed a rights-based approach to the management of data and technologies during crisis situations which includes the right to: be informed, protection, privacy and security, data agency and rectification and redress (2). These apply to contact tracing (3 ITWorld, Scassa) and to equity groups calling for demographic data (1). Other have conducted rapid response data reporting, for example after the Haiti Earthquake volunteers developed real-time crowdsourcing data collection systems to support humanitarian responders (4 Meier) and WeRobotics mobilizes local drone expertise to objectively assess proposed pandemic response technologies (5 WeRobotics).
This research will apply a critical data studies (CDS) theoretical framework (6 Kitchin & Lauriault), the principles of the HHI and, practice technological citizenship (7 Feenbert) to the study of the Canadian COVID-19 data response. Lauriault will leverage her expertise and Canadian and international network of open data, open government, civic technology experts in government, civil society, and Indigenous Communities (see CV) as seen in the policy briefs published on DataLibre.ca (8) to rapidly assess and support COVID-19 data management and reporting.
The objective is to carry out the following activities:
Compare official COVID-19 public health data reports to identify gaps and best practices (9 Lauriault & Shields).
Identify and support the building of framework datasets to standardize reporting (10 Lauriault).
Analyze data standards and protocols to support data management, interoperability and cross-jurisdictional reporting (11 GeoConnections).
Publish case-studies, resources, an archives of official reporting, and a glossary and
Rapidly conduct expert analysis, peer review, knowledge mobilization and provide evidence-based recommendations to improve data reporting.
The rationale for this research is as follows:
Official COVID-19 public health data are inconsistently reported, impeding comparability, and the ability to assess impact and target actions. Also, predictions missed seniors’ homes, precarious labour, and Indigenous communities and social determinants (12 Global News, NCCDH), resulting in an increase in cases and deaths. Currently job classifications and Indigenous, Black, and Racialized people classifications (13 CTV News) remain absent. This research will create a corpus of F/P/T and Indigenous Communities’ official reports, compare results, identify gaps.
Framework data are standard information infrastructures upon which other analysis can consistently be done (14 Toronto Star). When this is lacking analysis is impeded, for example there is no national reporting by health region since no national framework dataset exists (15 Lauriault), and mitigating the digital divide is thwarted with a lack of broadband maps (16 Potter & Lauriault et al.). Other missing national datasets include senior care facilities, homeless shelters, precarious labour, and Indigenous Communities (17 Gaetz et al.). Needed framework datasets will be identified and if necessary coordinate their building (18 SPCO, StatCan LODE), advocacy for the opening of public datasets such as corporate registries may be carried out (19 Fed. Registry, Open Corporate, Open Contracting), and experts from public health , social planning, and Indigenous Communities will help identify localized frameworks.
Consistent COVID-19 reporting requires an interoperable infrastructure which builds upon standards developed through consensus processes (20 CIHI, PHAC). Current uneven reporting may be attributed to a lack of standards adoption and formalization in terms of data flows. This research will develop a repository of standards and protocols and share these with decision-makers to improve interoperability (i.e. Data Standards for the Identification and Monitoring of Systemic Racism (21 ON Govt) and FNIGC OCAP Principles (22 FNIGC)).
Rapidly mobilizing knowledge is important to improve reporting and manage data, and to build a crisis data reporting infrastructure for the future. This project will compile, and archive information, rapidly assess and peer review results with experts and report results on DataLibre.ca and other websites, will produce infographics and policy briefs, deliver online webinars, and help administrators and Indigenous Communities improve their data and technology policies.
A CDS framework recognizes that data have social and material shaping qualities and that they are never politically neutral while also being inseparable from the people and institutions who create them including practices, techniques, and infrastructures. This involves a team of data, technology, legal, social and health, and Indigenous experts to rapidly assess official COVID-19 data assemblages and to act as technological citizens by applying knowledge in real time and mobilize results to mitigate the data shortfalls witnessed during this crisis and support decision makers to respond with a data humanitarian and rights-based approach for now and to better respond in the future.
Expected Impact:
The target audience for this rapid response data and technology reporting is F/P/T public officials and Indigenous Community Leaders who manage public health, socio-economic, statistical and official record data flows; and civil society actors and the public involved in open data, open government and open contracting, transparency and accountability. This includes C-class executives, chief technology, information data, and digital officers.
The outcome of this research is to standardize and improve humanitarian crisis data management and data reporting in the short term to ensure consistent reporting, and in the long term establish standardized data workflows and operationalize data infrastructures for this pandemic in preparation for the next.
The timing to compile, inventory and build an open access archives of official data reporting is now as the fractures in the system have become apparent in real-time and have had negative consequences. It is important to monitor the response as it evolves so as to be able to improve it while our collective institutional memory is fresh and to have the evidence available as a reminder for if and when we forget, but also to build more robust systems.
The results of this research will be continuously reported and made openly accessible as it becomes available and will lead to the formation of a new research team.
The following data and information were collected and analyzed by Tracey P. Lauriault, and Sam Shields a recent Carleton University Critical Data Studies graduate.
We set out to answer a very simple question inspired by a Twitter stream calling for COVID-19 reporting to include Indigenous, Black and Racialized characteristics. The following guided our activities:
What kind of demographic data are reported in official COVID19 reports?
On Thursday April 16, 2020 we spent the day searching the content of official government COVID-19 reporting sites. We compiled our data into a Google Spreadsheet, conferred over Skype, chatted in FB, and verified each other’s work. Official COVID-19 reporting dynamically changes as the pandemic evolves, and as institutions collect more data and build the capacity to report, they report more and they do so in a better way. I also consult experts in my network who comment and suggest resources. We will take another look next week to see if anything has changed. The following were our data sources
We found an incredible amount of information and overall, each province, territory and the Federal government make their data readily available and these are disseminated in charts, tables, maps, and dynamic dashboards and in daily surveillance reports. The data and indicators are explained, and data sources are generally provided.
In terms official COVID-19 reporting, there was very little reporting cases and outcomes with demographic variables and when there was, it is not standardized, making it difficult to do any national comparative analysis. Below is what we found.
1. Age
COVID-19 Cases by Age were reported by all provinces and the Federal Government. Age was not reported by all 3 Territories.
Those who did report, provided case counts and some percentages.
Only British Columbia, Alberta and Quebec reported Deaths by age groups.
Quebec reports age in 4 different ways.
There are no Age Range Reporting standards, and this impedes comparability.
The following is how COVID-19 Age data are reported, we ordered the results by similar reporting styles.
Sex is Not reported as a COVID-19 attribute, by 4 Canadian jurisdictions, namely the Territories and Newfoundland and Labrador.
For jurisdictions that do report COVID-19 databy sex, only binary classifications are used, Female and Male.
Only British Columbia, Alberta and Manitoba report Sex and Age as attributes.
Only Quebec and The Federal Government report Sex and Death.
Sex Variable Reporting Recommendations:
a)It is advisable to report COVID-19 indicators by sex such as Female, Male and Gender Diverse.
b)Sex disaggregated data are important in terms of informing testing; health interventions and it is associated with health outcomes. Knowing can inform planning.
c)Reporting age and sex is important as these are distinguishing characteristics in vital statistics, health, wellbeing, for longevity and death rates. Also, reports suggest that the virus affects men more negatively than it does women, especially older men. In terms of the labour force and COVID-19, nurses, doctors, elder care and home care professionals, those who work with people who live in group homes for the disabled and provide home care for these people, and people who clean these places tend to be women. Higher numbers of women are becoming afflicted by COVID-19 in Canada and this may be associated with their occupations. Age and sex are standard labour force statistical variables and reporting these attributes with COVID-19 will inform if health outcomes are related to those attributes.
3. Labour Classification
In official COVID-19 reporting, only the Provinces of Saskatchewan and Quebec reported any labour categoryand respectively they reported Case Counts for Health Care Workers for Saskatchewan and Cases Count and Death Count of Staff in hospitals and long-term care homes for Quebec.
b)The Canadian Institute for Health Information (CIHI) health workforce database includes standardized job classifications and data tables by job classification. They also have methodological guides comparing provincial systems. Harmonizing classifications across the provinces and the territories would go a long way to facilitating comparable analysis.
4. Indigenous, Black and Racialized People
No official government COVID-19 sites report data by any of these groups.
Race and ethnicity may or may not biologically predispose people to COVID-19 health outcomes. We are assuming that these data are being tracked but are not reported as there is a concern about how to report these data.
Indigenous, Black and Racialized people may also have preexisting health conditions that are socially and economically determined, and these preexisting conditions may disproportionally affect this group more than others. Furthermore, reports suggest that Indigenous, Black and Racialized People have been infected more than others, and their health outcomes are more dire. Evidence informed decisions can lead to better outcomes for some groups, reporting the numbers can advance better and more targeted practices in community, hospital and in our cities.
Recommendation on the Reporting with Indigenous, Black and Racialized People categories:
“guidance for race-based data collection for government and other public sector organizations, including steps to follow for data collection, management and use”.
Table 1. Valid Values for Race Categories on P.26 provides a useful classification system. The Standard also includes protocols for the collection of self reported or observed data.
b)First Nation, Metis and Inuit in Canada may be collecting these data in their communities. I will consult to see if that is the case and report back.
Final Remarks:
Health outcomes are intersectional, and age, sex, workforce and equity data provided additional insight about who is being affected, and knowing who and where can inform decisions about determinants of health, testing, improvement of health outcomes and planning. We have provided some insight in this post, about what is being reported and provided some recommendations. We will provide updates as more information is collected. We hope you find this useful and we welcome your comments and suggestions by email: tracey.lauriault@carleton.ca or on Twitter @TraceyLauriault.
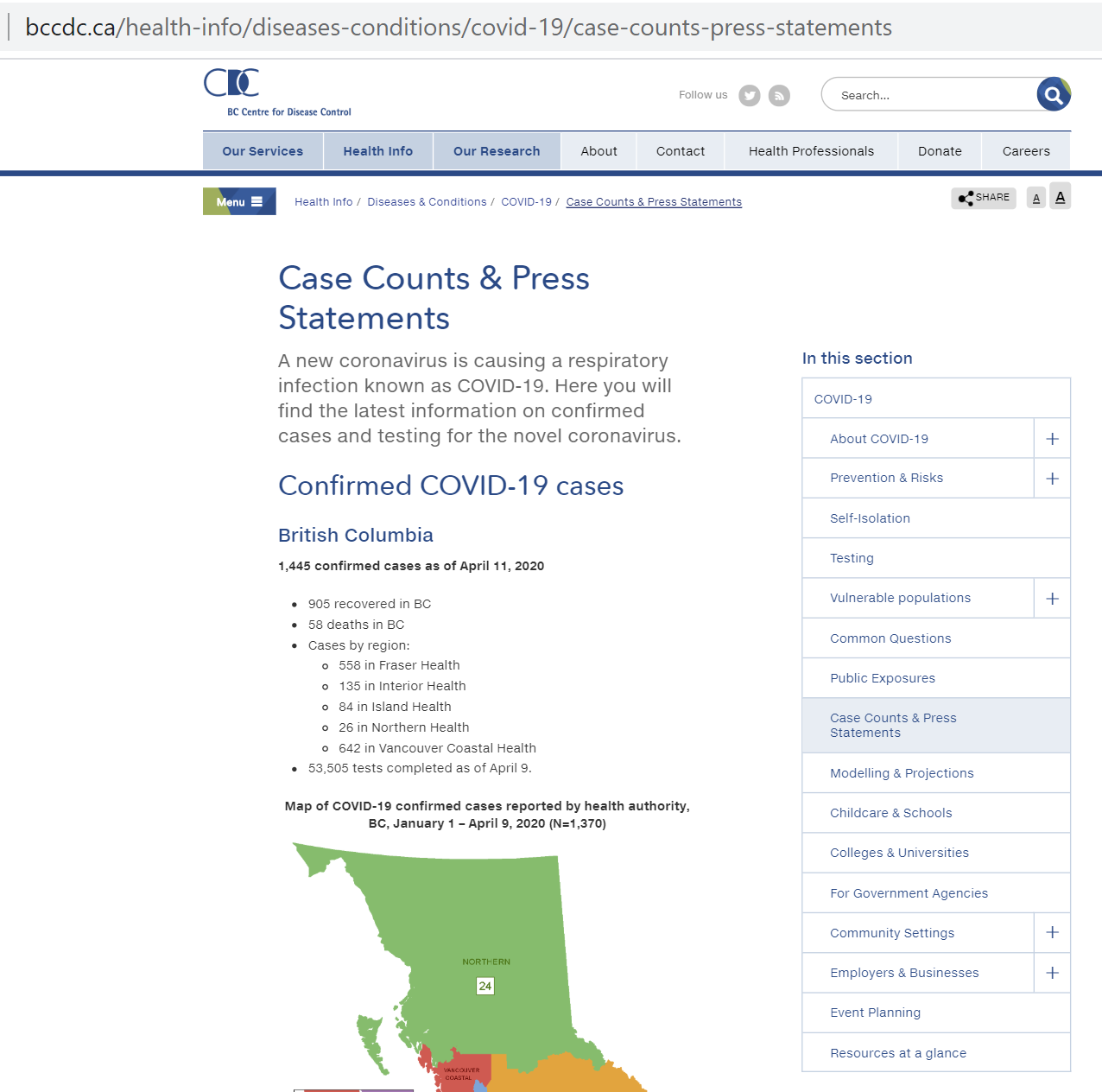
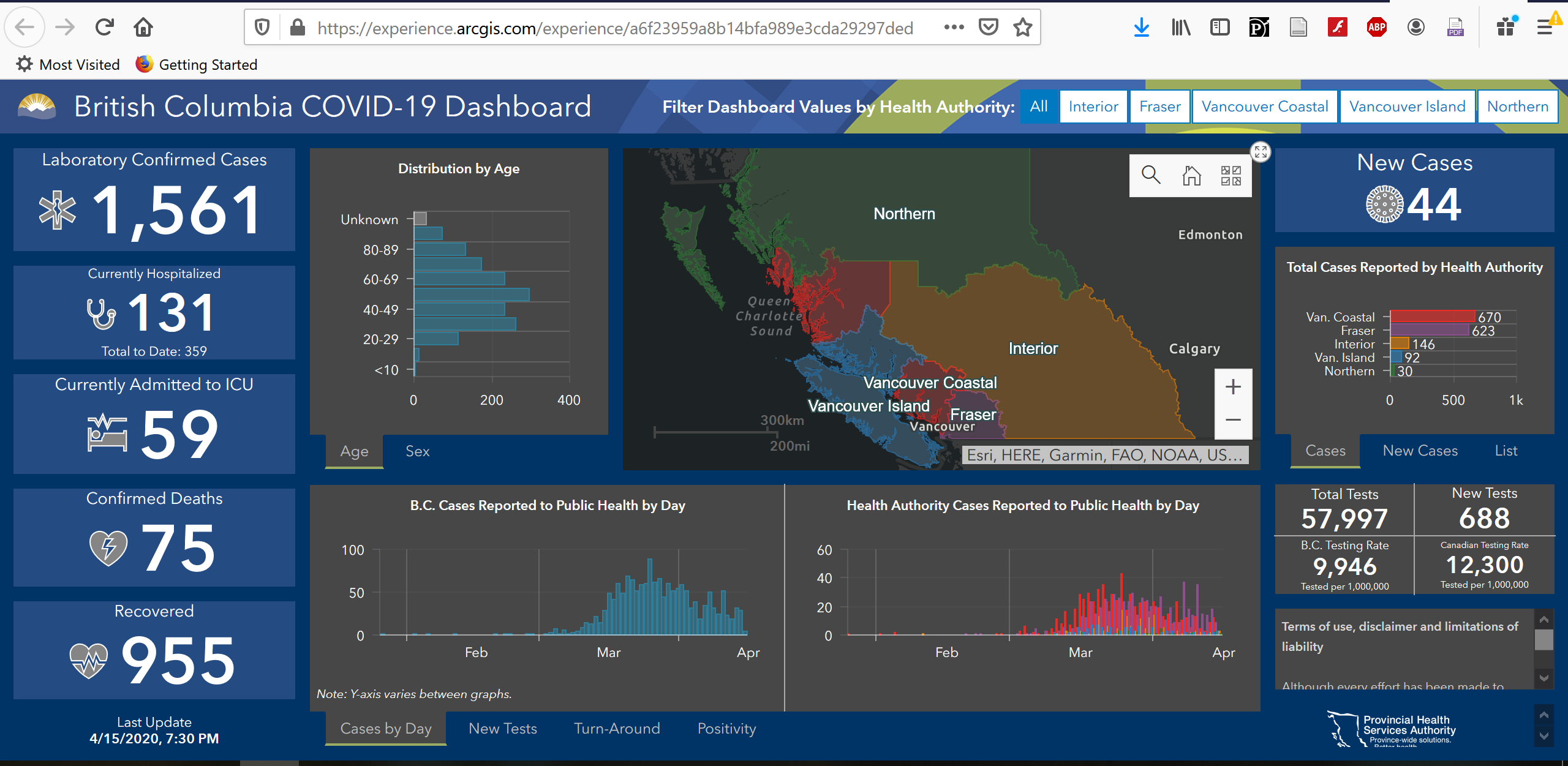
Reporting is becoming more sophisticated. The BC Centre for Disease Control (BCCCD) went from this landing page on the 13 of April, 3 days ago with data, maps, and charts as images on the page.
To this page today 16 of April and data are now reported in an ESRI dashboard, and some data available for download! I think it is easier to read. I hope they will continue to report their excellent Surveillance Reports, here is an example from April 15, 2020. You can access those reports at the bottom of the landing page. What is great about the dashboard is that it is a collaboration between a number of Provincial Agencies BCCDC, PHSA, B.C. Ministry of Health and GeoBC Production. Below the image I have also pasted what they include on their Terms of Use, Disclaimer and Limitations of Liability page from the Dashboard. The one issue with the dashboard, is you cannot download or link to specific pages.
Below I copied and pasted the information directly from the Dashboard at 9:45 AM EST, 16 April 2020. It is useful to have this all in one place, including access to data, data sources and notes about the indicators. This comes from the Dashboard, and unfortunately I cannot hyperlink directly to this information.
Terms of use, disclaimer and limitations of liability
Although every effort has been made to provide accurate information, the Province of British Columbia, including the British Columbia Centre for Disease Control, the Provincial Health Services Authority and the British Columbia Ministry of Health makes no representation or warranties regarding the accuracy of the information in the dashboard and the associated data, nor will it accept responsibility for errors or omissions. Data may not reflect the current situation, and therefore should only be used for reference purposes. Access to and/or content of this dashboard and associated data may be suspended, discontinued, or altered, in part or in whole, at any time, for any reason, with or without prior notice, at the discretion of the Province of British Columbia.
Anyone using this information does so at his or her own risk, and by using such information agrees to indemnify the Province of British Columbia, including the British Columbia Centre for Disease Control, the Provincial Health Services Authority and the British Columbia Ministry of Health and its content providers from any and all liability, loss, injury, damages, costs and expenses (including legal fees and expenses) arising from such person’s use of the information on this website.
BCCDC/PHSA/B.C. Ministry of Health data sources are available at the links below:
Click the top right corner of any chart/window to make it full screen. Click again to return to the dashboard view.
Data Sources:
Case Details and Laboratory Information Data are updated daily Monday through Friday at 5:00 pm.
Data on cases is collected by Health Authorities during public health follow-up.
Confirmed cases include laboratory positive cases.
Laboratory data is supplied by the B.C. Centre for Disease Control Public Health Laboratory; tests performed for other provinces have been excluded.
Data on intensive care unit (ICU) admissions is provided by the PHSA Critical Care Working Group.
Test and case values may differ between amalgamated Health Authorities and B.C. as site locations are confirmed.
Data Over Time:
The number of laboratory tests performed and positivity rate over time are reported by the date of test result. On March 16, testing recommendations changed to focus on hospitalized patients, healthcare workers, long term care facility staff and residents, and those part of a cluster or outbreak who are experiencing respiratory symptoms. The current day is excluded from all laboratory indicators.
The number of new cases over time are reported by the date they are notified to public health.
Epidemiologic Indicators:
Cases are considered recovered after two lab-confirmed negative swabs taken 24 hours apart or when removed from isolation 10 days after symptom onset.
New cases are those reported daily in the PHO press briefing and reflect the difference in counts between one day and the next as of 10:00 am. This may not be equal to the number of cases reported by day, as cases reported prior to 10:00 am would have been included as New Cases in the previous day’s count. Because of the 10:00 am cut-off, the most recent day in time series graphs may contain only partial information. On Mondays, the number of new cases includes the number of new cases from Saturday and Sunday.
ICU values include the number of COVID-19 patients in all critical care beds (e.g., intensive care units; high acuity units; and other surge critical care spaces as they become available and/or required).
Laboratory Indicators:
Total tests represent the cumulative number of COVID-19 tests since testing began mid-January. Only tests for residents of B.C. are included.
New tests represent the number of COVID-19 tests performed in the 24 hour period prior to date of the dashboard update.
COVID-19 positivity rate is calculated as the number of positive specimens that day/total number of specimens tested (positive, negative, and indeterminate) that day.
Turn-around time is calculated as the daily average time (in hours) between specimen collection and report of a test result. Turn-around time includes the time to ship specimens to the lab; patients who live farther away are expected to have slightly longer average turn around times.
The rate of COVID-19 testing is defined as the cumulative number of people tested for COVID-19/BC population x 1,000,000 population. B.C. and Canadian rates are obtained from the Public Health Agency of Canada’s Daily Epidemiologic update site.
Health Authority Assignment:
Health Authority is assigned by place of residence; when not available, by location of the provider ordering the lab test.
It is very odd that national health organizations are not reporting COVID-19 cases aggregated into health regions even though provinces and territories are mostly reporting them in that way. And where is the national health framework datasets?
Framework data are a “set of continuous and fully integrated geospatial data that provide context and reference information for the country. Framework data are expected to be widely used and generally applicable, either underpinning or enabling geospatial applications” P.7.
Federal Electoral Districts for example, are the official framework data for Elections Canada and these data are updated for each election. They are used to administer elections, report the results of exit polls during the elections, and show the results after an election. Framework data are available in multiple formats as well as in cartographic or mapping products for Geographic Information Systems (GIS) such as ESRI, MapInfo or Tableau (Shapefiles), in KML formats for GoogleMaps, and in standardized online mapping GML Formats which also happens to also be a Treasury Board Secretariat of Standard for Geospatial Data. Election result data are aggregated into these framework data along with other socio-economic data, and once these data are mapped we can compare and can tell a more nuanced local, regional and national story, we can see patterns across the country. The benefit of framework data are many, what is also great is they are created once by an authoritative source, they are updated and reliable, they are used many times, they are open data and everyone knows where to get them.
Considering that health care spending is one of the largest expenditures we have as a nation state, and it would be expected that in an era of accountability and transparency and where outcomes based management is the norm, it is astonishing that health data including its social determinants data are not disseminated in this way. Yes, there are privacy issues, but we are capable of addressing those with the Census and Elections, which means we can also do so for health. We need to have an evidence based conversation about population health now more than ever, and we will need these data to tell a socio-economic story as well. Could we have done better? Who is doing great and why and who is not doing so great and why, what can we learn and what is the remedy?
Numerous useful and insightful interactive maps were published after the elections (CBC, CTV, Macleans, ESRI and many others), and these generated much discussion, people could see the results, they could situate themselves, they could see what friends and family in other places were experiencing. Analysts and policy makers also had what they needed to understand and plan a new context. This is what democratic evidence based data journalism and policy making is all aboutt!
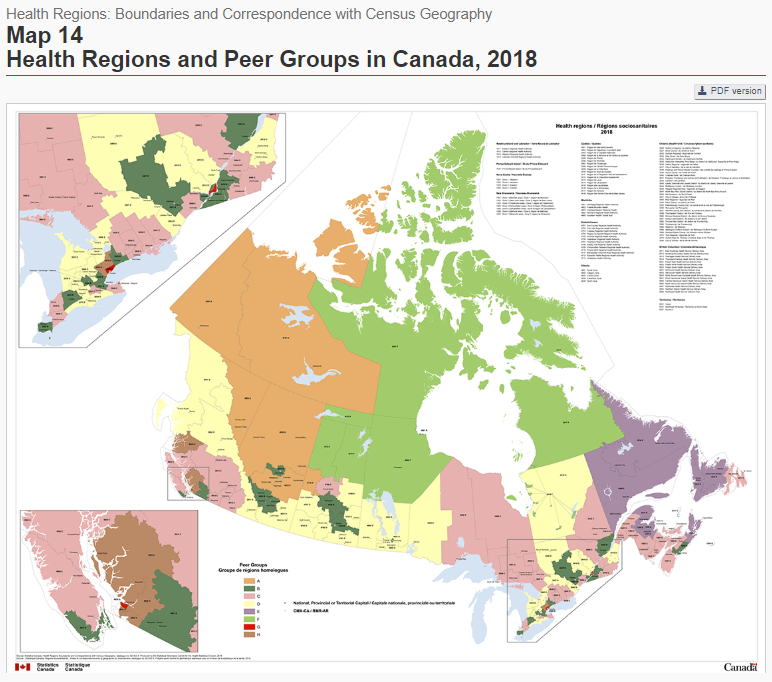
Natural Resources Canada is normally the producer of Canada’s framework data but it does not produce a health region framework dataset for Canada. Arguably, these data would not only be useful during a pandemic, but also for administering and reporting health associated with natural resources such as allergies in the spring and fall, food insecurity, health and farming, or health after a natural disaster such as flooding and fires. They data would also be useful to see where money is spent providing Canadians with the evidence they require to advocate for change.
So why no national heath reporting by their administrative boundaries and where is the health region framework dataset?
National Health Reporting Canada:
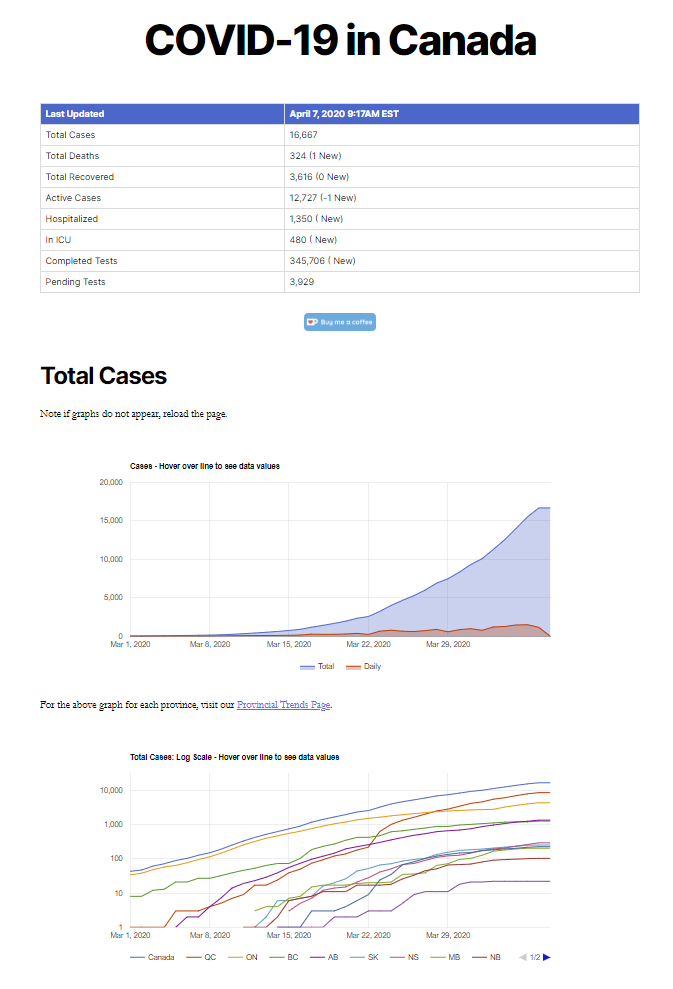
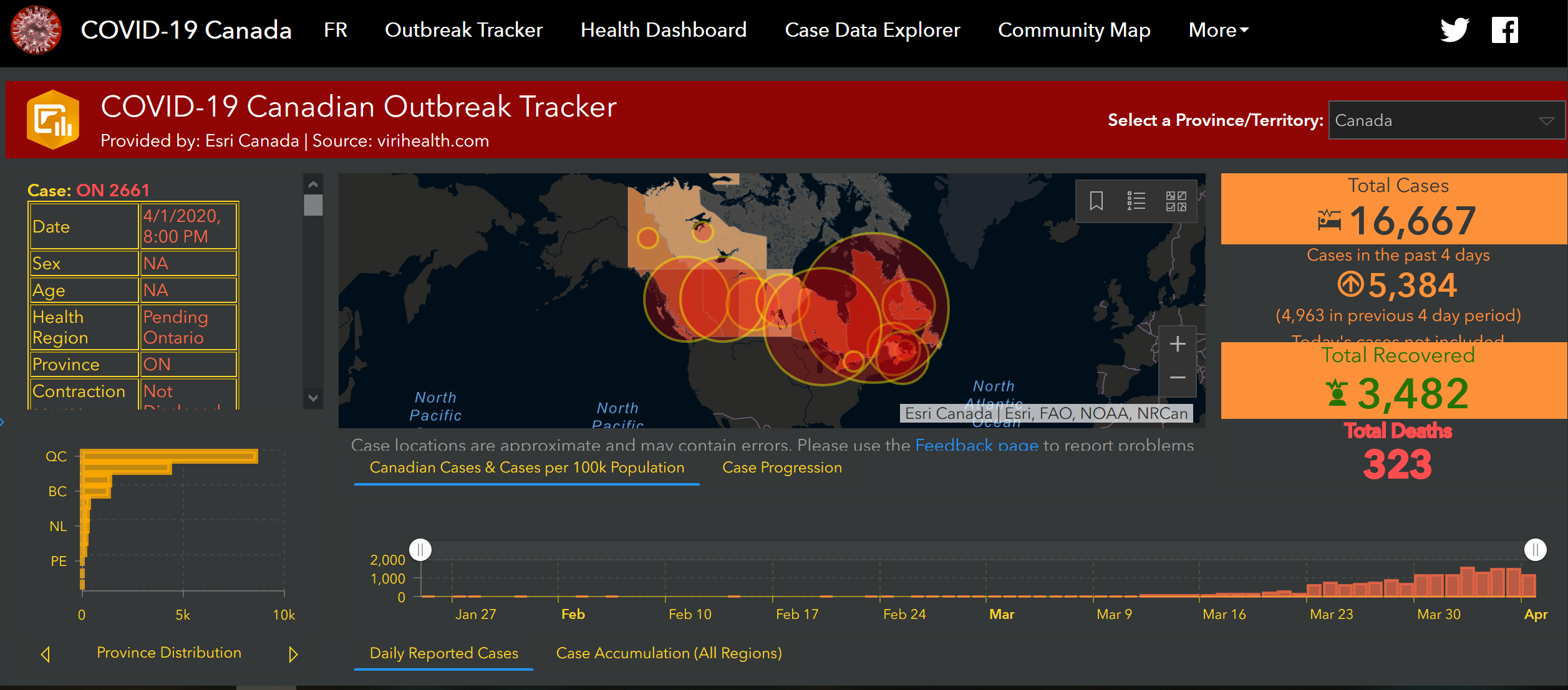
Virihealth.com and ESRI Canada produced the the first National ge0-COVID-19 reporting:
Canada as a federation has jurisdictional divisions of power, and one of those jurisdictional divides is health. We have the Canada Health Care Act (CHA) that
“establishes criteria and conditions related to insured health services and extended health care services that the provinces and territories must fulfill to receive the full federal cash contribution under the Canada Health Transfer (CHT)”.
The Canada Health Transfer (CHT) provides long-term predictable funding for health care, on a per capital basis and
“supports the principles of the Canada Health Act which are: universality; comprehensiveness; portability; accessibility; and, public administration”.
The provinces and territories receive cash transfers to deliver health care to Canadians and health care data reporting is done by the each province and territory separately. This alone justifies the creation of a national health region framework dataset. Which organization should be responsible for it?
There are three main organizations which are part of the Canada Health Portfolio that currently report official COVID-19 cases. At the moment, they do not publish COVID-19 case data by health regions.
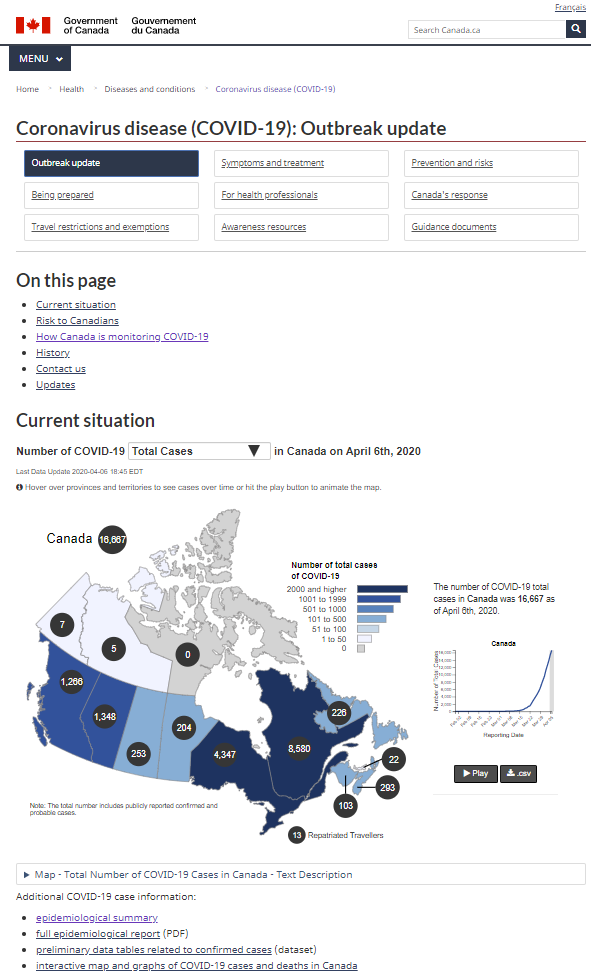
Health Canada “is the Federal department responsible for helping Canadians maintain and improve their health, while respecting individual choices and circumstances.” Health Canada is an official and authoritative national source of COVID-19 data and it publishes the Coronavirus disease (COVID-19): Outbreak update. Reporting includes an interactive map and a line graph of data by Province and Territory.
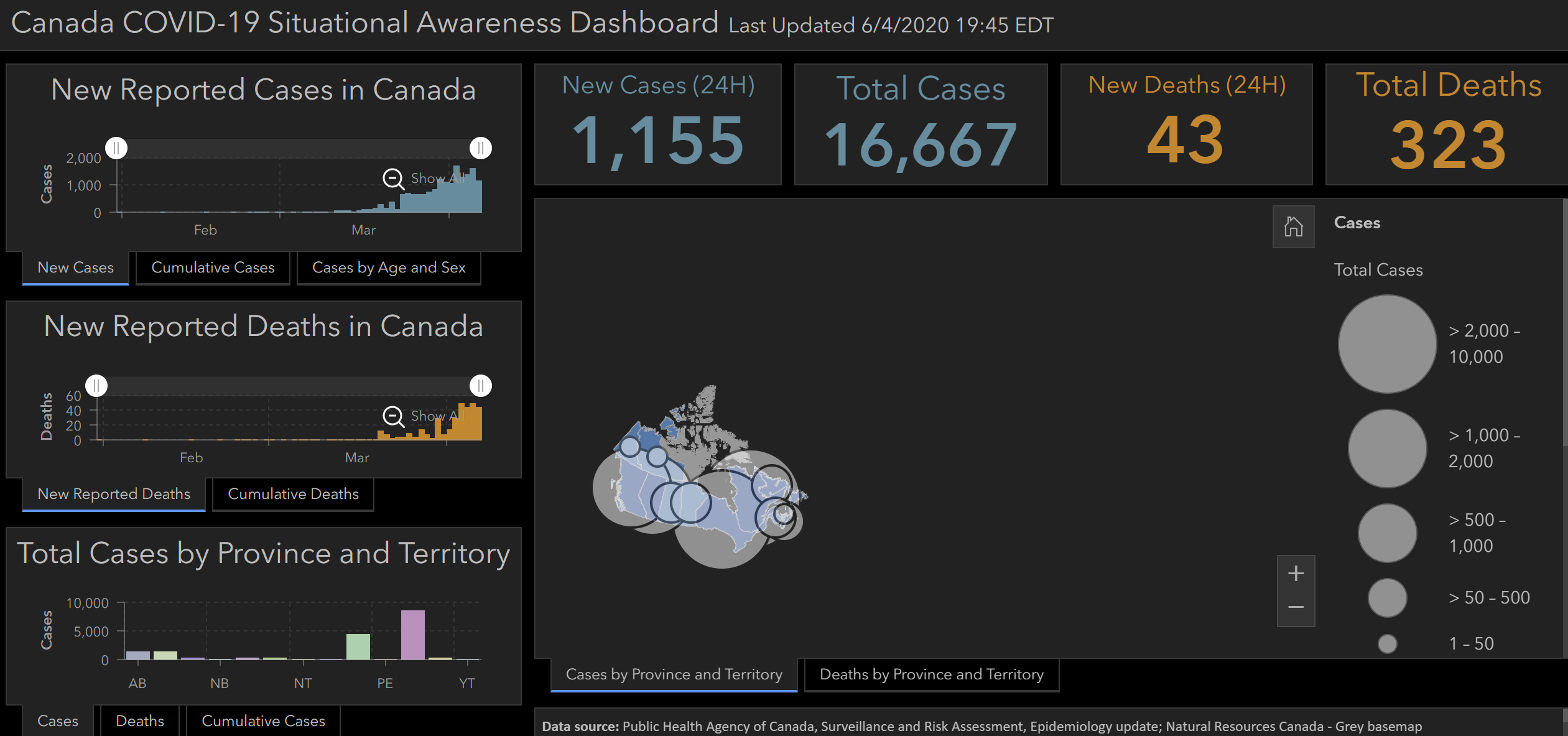
Public Health Agency of Canada (PHAC) promotes and protects the health of Canadians through leadership, partnership, innovation and action in public health and it does so by: Promoting health; Preventing and controlling chronic diseases and injuries; Preventing and controlling infectious diseases; Preparing for and responding to public health emergencies; Serving as a central point for sharing Canada’s expertise with the rest of the world; Applying international research and development to Canada’s public health programs; and Strengthening intergovernmental collaboration on public health and facilitate national approaches to public health policy and planning. PHAC now disseminates an excellent interactive dashboard entitled the National Epidemiological Summary of COVID-19 Cases in Canada. Their data sources are: Public Health Agency of Canada, Surveillance and Risk Assessment, Epidemiology update; Natural Resources Canada – Grey basemap with Credit: COVID-19 Situational Awareness tiger team Powered by ESRI-Canada and COVID-19 Canadian Geostatistical Platform, a collaboration between Public Health Agency of Canada, Statistics Canada and Natural Resources Canada.
Canadian Institute for Health Research (CIHR) is the Government of Canada’s health research investment agency and its mandate is to “excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health care system.” Although a research funding organization, CIHR could publish a national framework dataset of health units to help researchers in Canada and to also to disseminate the findings of research either about COVID-19 or any other research according to those administrative boundaries. (Update 07/04/2020 CIHR does not have a framework data file)
A national non-governmental organization, the Canadian Institute for Health Information (CIHI) also disseminates national comparative health data, mostly about the administration of health and it would make sense for them to also publish data by health units and to have such a framework dataset. CIHI is an independent, not-for-profit organization that provides essential information on Canada’s health system and the health of Canadians. (Update 07/04/2020 CIHI does not have a framework data file). CIHI’s mandate is
“to deliver comparable and actionable information to accelerate improvements in health care, health system performance and population health across the continuum of care”.
Natural Resources Canada is the producer of most of Canada’s Framework data, and it could with the help of the Canadian Council on Geomatics Provincial and Territorial Accord could create this framework file and this was discussed at the 4th Annual SDI Summit meetings hosted in Quebec City in the Fall of 2019.
Provincial and Territorial Official COVID-19 Case Reports and health geographies:
Below I have compiled a list of official COVID-19 Case reporting by province and territory, and when I could find them, I included a link to health administration geographies. That does not mean that data are reported in maps, but data are generally tabulated according to health administration geographies.
NB has two regional health authorities (RHAs) as explained in their Health Act and has, in addition to the RHA structure, seven health regions for purposes of the Act.
Informations concernant les limites territoriales : des réseaux locaux de services (RLS), des centres locaux de services communautaires (CLSC), des réseaux territoriaux de services (RTS), des régions sociosanitaires (RSS) et les réseaux universitaires intégrés de santé (RUIS)
I have emailed each of the Provincial and Territorial governments to confirm that I have the latest heath geography framework data. I have received updates from Yukon, Quebec, PEI, New Brunswick, and Manitoba, and have updated map data accordingly. I have also received correspondence from Statistics Canada, and CIHI.
For the moment ESRI Canada and some of the Provinces and Territories are reporting Official COVID-19 Cases by health region geographies. Why aren’t Health Canada and the Public Health Agency of Canada doing so? And where is the National Health Region Framework Data file?
Across the country adhoc open data groups are meeting, holding hackathons online, they are making all sorts of apps, they are asking for data and want current data channels improved, they are making maps and deploying platforms, but also they are concerned about tracking and surveillance. These groups involve people from all levels of government, civic technology, open data, and the private sector. People are involved for all kinds of reasons and what is notable is that these are people who have agency, knowledge, and power combined with the capacity to act – the key ingredients for what Andrew Feenberg would call, technological citizenship. Doing technological citizenship is one way for people to engage in a technological society such as Canada, and in a very sophisticated and complicated information and technology situation such as a pandemic.
People’s intentions are good, but as the saying goes ‘the road to hell is paved with good intentions’ and caution and level headedness is required.
It is time to bring this overseas humanitarian crisis work home!
This is an exceptional time and right now we are witnessing the erosion of basic rights in exchange public good, as the situation is ‘evolving’, while a new form of data politics emerges with little or no discussion of data governance. The changes comes with an increase in surveillance and control, which might stay longer than we had thought and hoped for.
This too is not new, and the Signal Code work was developed precisely for this type of situation. These researchers advocate for a rights based approach for humanitarian information activities (HIA) work during a crisis, a pandemic is arguably a crisis, and they refer to the Humanitarian Charter and Minimum Standards in Humanitarian Response that starts with an understanding of dignity as being:
…more than physical well-being; it demands respect for the whole person, including the values and beliefs of individuals and affected communities, and respect for their human rights, including liberty, freedom of conscience and religious observance.
They also argue for a duty of care to be operationalized during the crisis, and I would argue that this should be done by us and our governors and administrators, so that we do not use this pandemic as reasoning to violate rights, to circumvent the law and to be negligent in our data and technology work. The COVID-19 pandemic is temporary, but the data collected and the technologies built will live beyond the crisis. There therefore a duty to be responsible now and to develop data governance strategies for the future.
The goal of the Signal Code is to develop ethical obligations for humanitarian actors including minimum technical standards for the safe, ethical, and responsible conduct of humanitarian information activities (HIAs) before, during, and after disasters strike. They provide the following five rights when conducting HIAs:
1. The Right to Information
Access to information during crisis, as well as the means to communicate it, is a basic humanitarian need. Thus, all people and populations have a fundamental right to generate, access, acquire, transmit, and benefit from information during crisis. The right to information during crisis exists at every phase of a crisis, regardless of the geographic location, political, cultural, or operational context or its severity
2. The Right to Protection
All people have a right to protection of their life, liberty, and security of person from potential threats and harms resulting directly or indirectly from the use of ICTs or data that may pertain to them. These harms and threats include factors and instances that impact or may impact a person’s safety, social status, and respect for their human rights. Populations affected by crises, in particular armed conflict and other violent situations, are fundamentally vulnerable. HIAs have the potential to cause and magnify unique types of risks and harms that increase the vulnerability of these at-risk populations, especially by the mishandling of sensitive data.
3. The Right to Privacy and Security
All people have a right to have their personal information treated in ways consistent with internationally accepted legal, ethical, and technical standards of individual privacy and data protection. Any exception to data privacy and protection during crises exercised by humanitarian actors must be applied in ways consistent with international human rights and humanitarian law and standards.
4. The Right to Data Agency
Everyone has the right to agency over the collection, use, and disclosure of their personally identifiable information (PII) and aggregate data that includes their personal information, such as demographically identifiable information (DII). Populations have the right to be reasonably informed about information activities during all phases of information acquisition and use.
5. The Right to Rectification and Redress
All people have the right to rectification of demonstrably false, inaccurate, or incompletedata collected about them. As part of this right, individuals and communities have a right to establish the existence of and access to personal data collected about themselves. All people have a right to redress from relevant parties when harm was caused as a result of either data collected about them or the way in which data pertaining to them were collected, processed, or used.
These are important to consider. I will come back to these in the coming days and I will point to insight provided by other who have first hand experience of doing data work during a time of crisis. I hope this is food for thought.
Both Hugh and I agree, that it is time to use this platform again.
COVID-19 and cell phone data tracking is a Privacy Paradox par excellence! The the concept originally encapsulated how we were willing to trade-off the sharing of one’s data for the use of a ‘free’ social media platform. We kinda’ knew that our data were being sold off to third parties, and traded by data brokers, and we sorta let it go, so we reacted by setting up some add blockers, adjusting our settings, using VPNs, or changing our browsers to things like DuckDuckGo. As imperfect as that situation was and is, that is what we did and it is what we do.
But cell phone tracking is something quite different.
Helen Nissembaum‘s Contextual Integrity (CI) is a very useful framework to think this through, for her “privacy, defined as CI, is preserved when information flows generated by an action or practice conform to legitimate contextual informational norms; it is violated when they are breached“. There are four CI theses as follows:
Thesis 1: Privacy is the Appropriate Flow of Personal Information
Thesis 2: Appropriate Flows Conform with Contextual Informational Norms (“Privacy Norms”)
Thesis 3: Five Parameters Define Privacy (Contextual Informational) Norms: Subject, Sender, Recipient, Information Type, and Transmission Principle
Thesis 4: The Ethical Legitimacy of Privacy Norms is Evaluated in Terms of: A) Interests of Affected Parties, B) Ethical and Political Values, and C) Contextual Functions, Purposes, and Values.
In terms of norms, social media is one thing, we do get upset when we find out that our photos are being used for facial recognition by our law enforcement institutions, when behaviour is tracked for targeted marketing purposes by data brokers or worse when scurrilous actors use our data to disrupt democracy. But our cell phone data, that is another level! We also know about UBER and smart phone provider transgressions but we seem to know very little about the Murkyness of Telecom Surveillance. Furthermore, we are beginning to realize, that we cannot Privacy By Design (PbD) our way out of this, nor is cybersecurity enough, and that institutional and technological solutionism, falls short! We need to figure out how to govern these data practices right now.
These are exceptional times, circumstances are exceptional, the stakes are high, and the norms they are a changin’ . CI helps frame our thinking, although, Nissembaum also realizes that her thesis may need to reconsider how technology is an actor, while Teresa Scassa in Private Sector Data, Privacy and Pandemics and Michael Geist both warn us about the new normal, they also define and categorize types of data in a pandemic situation to help us out, frame their analysis with issues pertaining to law, policy and governance, and provide ways to circumscribe how these data might be shared to serve the public good or interest at this time.
But, who will govern this, and for long will this ‘sharing’ & tracking go on for?
What is for sure, just like 911 set new benchmarks in terms of what kind of surveillance we wound up ‘living with’, COVID-19 will change data and technological monitoring norms. This may also be a time where we might change the course what surveillance we will accept, as presumably we are smarter now! There are perils and there are opportunities. How will we govern ourselves and our data during and post the pandemic era!
Below is a smattering of news articles on the topic:
datalibre.ca is a blog, inspired by civicaccess.ca, which believes all levels of Canadian governments should make civic information and data accessible at no cost in open formats to their citizens. The data is collected using Canadian tax-payer funds, and we believe use of the data should not be restricted to those who can afford the exorbitant fees. [more…]
Email: contact AT datalibre DOT ca


Comments on Posts